When your baby is born and something isn’t quite right, you enter a world you never expected to be part of. A world filled with medical terms, unfamiliar equipment, and questions you didn’t think you’d ever have to ask.
One of those terms might be duodenal atresia. And if it is, you’re not alone. You’re not expected to understand everything right away.
Let me help you begin.
What is duodenal atresia?
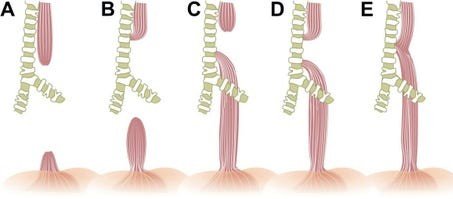
Duodenal atresia is a condition some babies are born with. It means that the first part of their small intestine, called the duodenum, didn’t form completely. There is a blockage that makes it impossible for food or fluid to move from the stomach into the intestines.
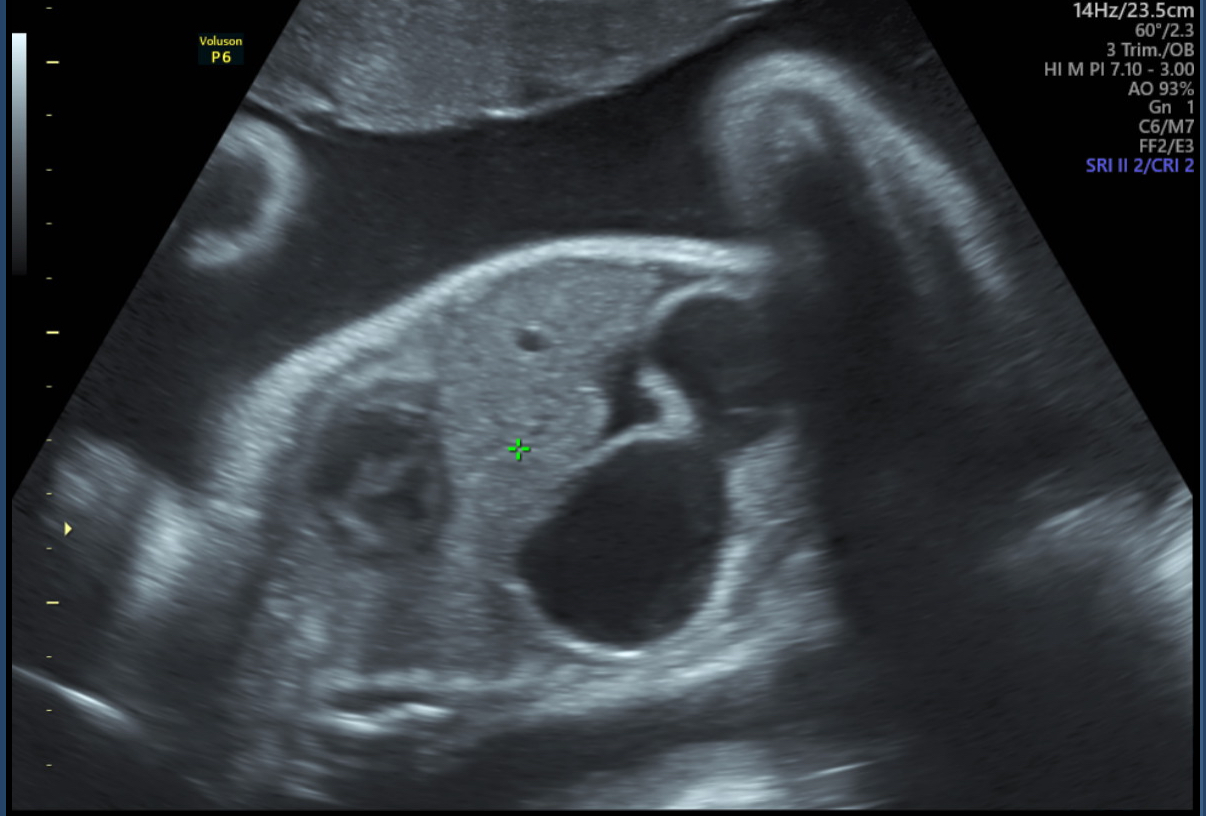
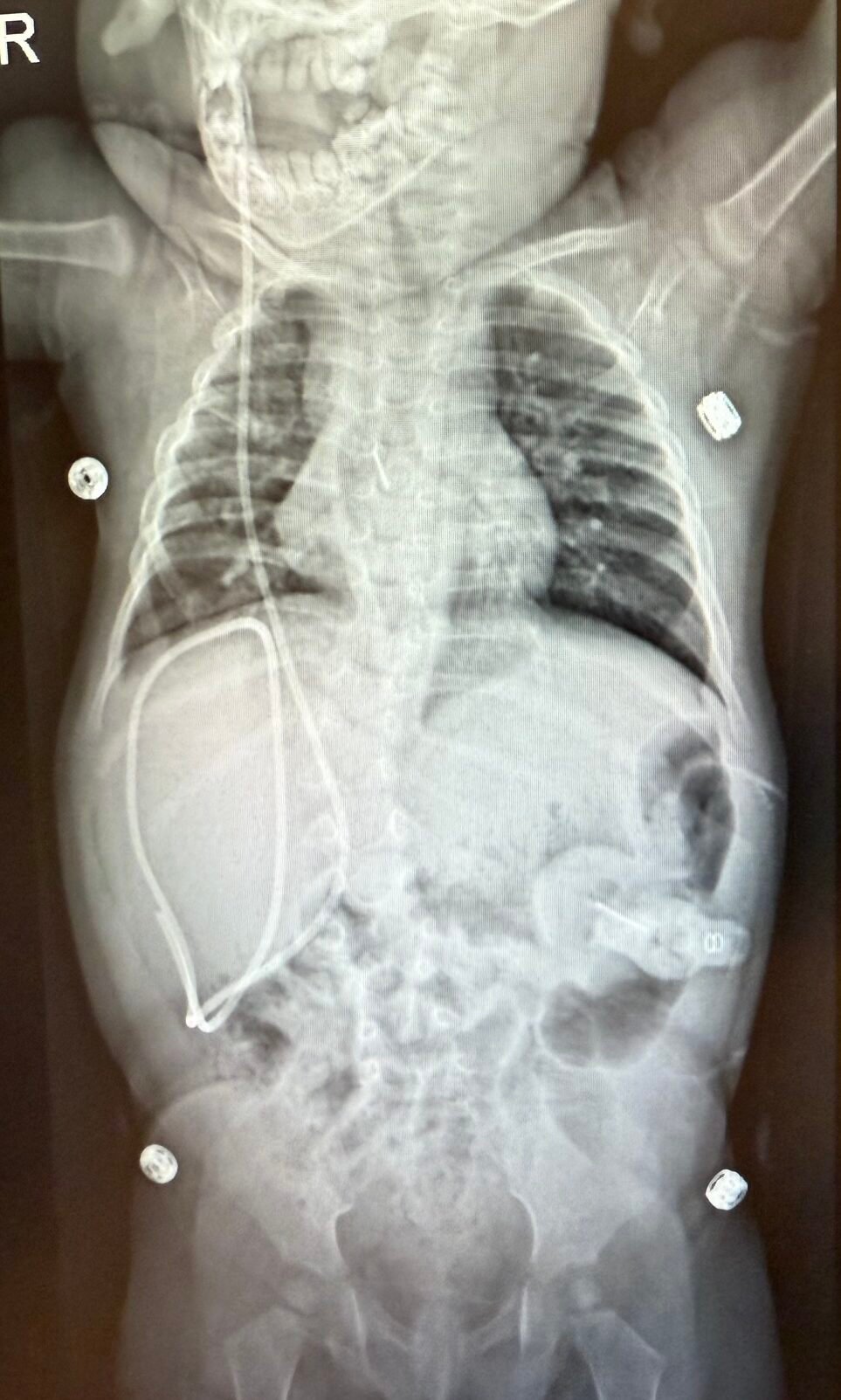
Because of that blockage, babies with duodenal atresia often vomit shortly after feeding. The vomit can be green, due to bile. Some babies are diagnosed during pregnancy through ultrasound. Doctors may see a swollen stomach and duodenum — also called the “double bubble.”
How is it treated?
Duodenal atresia cannot fix itself. It always requires surgery. A pediatric surgeon will connect the two healthy parts of the intestine so that milk and food can pass through again. This surgery usually happens in the first few days after birth.
After surgery, your baby may not eat right away. Instead, they may receive nutrition through an IV while the body heals. When the time is right, feedings are started slowly, often with a feeding tube. Recovery takes time, but most babies do very well.
What does this mean for you?
This is a lot to take in. One moment you’re picturing quiet feedings and newborn snuggles, and the next, you’re talking about hospitals, surgery, and long nights.
If you’re scared, that’s okay. If it hurts, that’s normal. And if you feel like you don’t know how to do this — know that I felt the same.
But you will learn. You will hold your baby through it all. You’ll ask the right questions. You’ll be stronger than you thought possible.
Your baby is more than their diagnosis. And you are more capable than you feel right now.